










When I started working in a nursing home in 2014, I had very little understanding of what was required from me in providing meals in an aged care facility. I was aware that 49 residents needed meals throughout the day and at the time we had 18 people on modified diets. The brief was, to present all the meals in the best way possible.
Each service was extremely busy as all meals were plated in the kitchen from their menu choices and very little interaction between the kitchen and the resident. We simply didn’t know our residents! We knew that we had 49 residents, with 12 on an IDDSI level 4 diet and 6 on an IDDSI level 5 diet, 5 of whom were Diabetics and 2 high cholesterol, but we did not know who they really were.
My name is Niamh Condon and I am the Head Chef in a Nursing Home in Co. Cork, Ireland. Here we have achieved a level 1 in the Dementia Care Matters Programme for the last 3 years running and are very passionate about the care our residents receive.
With a background in the hospitality industry from the age of 12, I have gained a lot of varied experience from butchery, deli’s, hotels, restaurants and running my own business in events catering. This has thought me to adapt and evolve with each new role and pushed me to learn as best I could.
I don’t profess to know it all, but I can give you some information on how I made changes in the lives of our residents. We are not trying to reinvent the wheel and I’m not about to tell a chef how to cook a beef casserole but to give tips on how to improve the way that we serve our modified foods.
In my head, I thought this was madness….
Little changes in your daily dining routine can make all the difference.
So, what did I do? I could see that these people depended so much on the social interaction that mealtime provided, so we got involved.
How do you do that? You might say. Little changes to your daily routine can make all the difference. At first, there was little resistance from the catering staff as they felt that this was extra work and that it would benefit nobody. Over time I gained the trust of the catering team and the nurses as they were witnessing mealtimes as a happy interaction and residents were looking forward to their meals.
How did this happen? I encouraged the kitchen staff to serve each resident as if they were in a restaurant and got to know their names, likes and dislikes, their special dietary requirements and preferences. But we still found that the residents that were on a modified diet were not getting the same attention and their plates looked less appealing. 3 scoops of different coloured food on a plate would not entice anybody to eat it. Often this was scraped into the bin.
I found that taking full control over the dining experience resulted in positive changes.
We then changed the colour of our uniforms to enhance positivity and mood. (white was very clinical and black a tad morbid…. Not ideal where we work)
The choice was very limited in the modified foods as there wasn’t enough information about what foods blend well. This was all trial and error and it pushed the kitchen staff to want to learn more.
Again, there had to be a better way!
So, we tried piping the modified foods onto the plate which resulted in the resident being able to choose the meal they preferred as their choice was visual. This was encouraging and we developed it a bit more. We then progressed onto using moulds and with the combination of using both methods, of piping and moulding the food, our residents were eating more.
Our next challenge was to reduce the dilution rate of the food because when you blend a solid food you must add liquid to get the required consistency depending on the food.
For example, a chicken fillet would need more liquid than Carrot to blend.
What I didn’t want was, to have food on a plate that had no nutritional value!
So now the big question….
Taste….
What happens to your mouth when you look at this?
 The picture speaks for itself!!!
The picture speaks for itself!!!
Your mouth waters….
Why is sight involved in taste…… well you’ve just seen why? It gets the mouth ready for the food that it is about to consume, by activating the salivary glands. We don’t have to eat an orange to know that it’s orange. We associate the smell and appearance. If the food does not represent the colour and shape, we are used to, we are likely to refuse it. I’m not going to go into too much detail about the chemistry of taste but like everything in life, 1st impressions!!!!
So now what happens if you are faced with this????
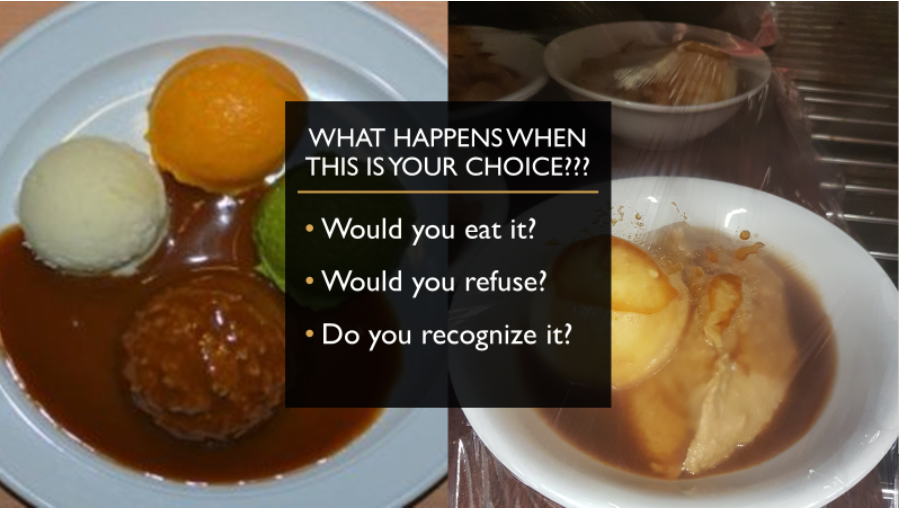
Would your mouth water?
This is some form of a beef casserole and a lamb stew….
Appetising? I don’t think so.
But again, this is standard, in most care homes as we are more concerned with the correct texture than anything else… but there is so much more to taste.
The temperature of the foods can influence us to eat the meal as hot meals smell delicious…. Cold salads only entice us to eat them if they look appealing
I’ve seen pureed chicken, potato salad and egg mayonnaise on the same white plate from 8oz potato Scoop and people refuse to eat it….
And then with a little imagination, we can create this…
 Beef Casserole with beef in cubes, carrots, peas, potatoes, and gravy
Beef Casserole with beef in cubes, carrots, peas, potatoes, and gravy
And the use of coloured plates makes the food stand out especially for those suffering from dementia.
Some of what is on the plate were prepared the day before (frozen carrots) Beef puree was created using a gelling agent and set in a flat tray, cut into squares to resemble cubed pieces of meat and the peas were piped, the potato was scooped and cut in half. This dish was ready for IDDSI level 4 diets and served with a thickened sauce to resemble a casserole. So, with a little preparation and imagination, you can create all sorts of beautiful plates of foods.
 Here we have a Fruit Salad…. Prepared a day in advance
Here we have a Fruit Salad…. Prepared a day in advance I want to prove to people that you can prepare meals at home and make them presentable without the use of moulds but also to have a combination of moulds and piping techniques that can make very attractive plates of food.
The only limit to plating foods is your imagination and unwillingness to learn.
Residents’ reactions to these foods were amazing. One would have to witness the facial expressions of people when they see, smell, touch and taste these foods….
It is very Humbling!!!
The Catering team was blown away by the positive feedback from relatives, care staff, nurses and dietitians. Their loved ones were happy at mealtimes, knew their chefs, servers, gaining healthy weight from the foods now being produced. Carers were finding it easier to assist with meals as the residents were eating and loving their foods. Nurses and dietitians were happy that there was very little weight loss and the nutritious meals encouraged muscle growth and healing.
I now had the interest of the catering team to learn more!
So, we are back at taste….
And specific flavours Sweet Sour salty bitter and savoury.
Some people prefer sweet some prefer savoury…. It is important for other residents, staff & family members to be involved as much as you can. We need to encourage all stakeholders to view the dining experience as positive.
So how do we change?
 Finding out a person’s likes and dislikes and discussing it with the Speech & language therapists and dietitians to see what they would prefer, and this helps to come up with a meal plan for the individual….
Finding out a person’s likes and dislikes and discussing it with the Speech & language therapists and dietitians to see what they would prefer, and this helps to come up with a meal plan for the individual….
Menu planning is important as it is cost-effective and less waste with more consumption
For example, we have Roast beef for dinner with Carrot & parsnip, so we prepare this for a beef casserole for the following day’s tea! Plan….
Like Benjamin Franklin said ‘fail to plan is planning to fail’
If so, training the person that is assisting, in giving the food as it is intended and not mixing everything up on the plate because it’s easier! Where the carer believes it’s the same thing anyway??? NO, IT’S NOT!! If I have this fruit salad, and you mash it up and taste it, can you tell me what you’re eating? Or if I give you a piece of kiwi and then a piece of strawberry can you identify with your foods? Yes, because they are now familiar…. you can now see them and taste them individually!
Initially, using food moulds, I found it easier to give the correct portion size to a person rather than freehand piping. And this also ensured that the person was not facing a huge amount of food on their plate which can be off-putting.
When we start to suffer from medical conditions such as dementia, taste disorders, acquired brain injuries, other neurological conditions, or advanced age, our taste sensations change, cravings occur and additionally, as we age, our taste buds and sense of smell diminish. What we once enjoyed may no longer hold any appeal. This can make the mealtime experience unpleasant and cause a rapid decline in consuming the necessary nourishment our bodies require.
Some of our Residents who are in their 90’s are now enjoying chicken curry and rice but would never have eaten this in the past.
It’s all about finding the right balance and meal plan to suit the person. Also, other things to take into consideration…. does the food need to be fortified if they are eating only a small portion?
So, does it need calories? Protein? Fibre (obviously Soluble) or other nutrients and then we must learn how to incorporate this into the food.
Also, you may need to give an individual smaller more frequent meal.
You may have to give finger food to a person with dementia as they may not sit for a meal but continue to walk around. People with dementia require more calories as their brains are overactive and they burn more. They also develop a very sweet tooth (which is probably why the supplements are sweet and so popular)
I have observed how difficult it is to glamorise smooth puree foods and as a chef, we are thought to have different textures on a plate, so it goes against what we have learnt. Facing with this texture many people become disinterested in eating, excluded from the mealtime experience, isolated and typically malnourished as a result.
So, we found that adding certain ingredients to the blended food would increase our nutritional content, especially for those whose appetites would be small, and large portions would be off-putting.
There are lots of ways to increase the nutritional value of the foods that we are preparing and if there was proper training on this, I believe our residents would be healthier and less agitated.
Also important is for all carers and kitchen staff to be trained on heating the foods as they are very delicate, and they can be easily overheated in microwaves and combo ovens.
Textured foods need to be fully covered and an airtight seal, especially as steam can add extra water to the foods and make them collapse and unpleasant. As it is reheating the temp only needs to reach 70 degrees and kept hot above 63 degrees
It is also important to bear in mind that the food cannot spend too long in a hot unit. This can result in crusty edges of the food.
Mealtimes are a time for social interaction in all of our lives, so a person with a swallowing difficulty might find it isolating when in a social gathering. They may feel that they can’t have the same foods and are afraid to ask for items to be blended as this is seen as childish. This is where all chefs in all areas of Hospitality should be able to prepare a meal [LINK TO MEALS ON WHEELS] for somebody suffering from dysphagia and have a greater understanding of the difficulties that the individual may have.
My challenge is to have the meal looking picture perfect by the time the resident receives it. Yes, it can be done but more and more training is required along with time, care, attention to detail and an understanding of the process.
YES!!!! Moulding the foods is important but not the total solution as we simply need to think outside the box!!!!
At the end of the day, we eat with our eyes first, so if something is more appealing to look at, we are more inclined to try it. It is up to us to get the resident eating and enjoying food to maintain a healthy life.
My goal is to ensure that in every restaurant and bar, hotel & café that there is an option to have a texture modified meal available and to educate the chefs on the importance of this. Afterall we are an aging population.
1st thing I noticed is that there was more communication between staff when they realised that we can give better plates of food to our residents. They were more interested and willing to help, by giving you feedback as to whether the resident liked or disliked their meal
They will also give ideas and suggestions as to what to cook next and ask you to try new recipes….
Which leads to good staff morale…. Team building and positivity in the home which rubs off on the residents
According to Dr. Aoife Ryan:
“Malnourished patients are at much greater risk of infection, are much more likely to be admitted (and re-admitted) to hospital and are at high risk of mortality compared to well-nourished patients.
Scientific evidence consistently shows that providing good nutritional care to these patients improves their health outcomes and reduces health care costs. Good nutritional care is, therefore, a critical component of good medical care.“
 If we were trained correctly on thickening drinks, it may encourage people to drink more. Thickened water is horrendous, so finding a drink that is nutritious and tasty may be beneficial to preventing dehydration. Watermelon slushy……
If we were trained correctly on thickening drinks, it may encourage people to drink more. Thickened water is horrendous, so finding a drink that is nutritious and tasty may be beneficial to preventing dehydration. Watermelon slushy……
More kidney function can decrease UTI’s as drinking fluids ( not caffeinated) can help flush bacteria out of the system
If we can give the resident the food that they like and will eat, it means that they won’t be agitated from hunger.
I firmly believe that training the catering departments, on dysphagia and how to present foods more appealingly, will give only give positive results. There would also need to be a form of monitoring this as currently there is not.
Chefs are competitive by nature, so if there was an award scheme for all of this and a small bit of recognition, it would certainly be an incentive to achieve more!
What I really would like to stress to all who work in Care Homes is:
I finally found my Mojo with Food!!!
I always thought that my dream job was to have a delicatessen style coffee shop with a fast-paced daily routine, where the focus was on good food presented well.
But it wasn't until, they needed a relief chef in the local nursing home, that I fell in love with food from a different perspective.
From cooking food because people wanted a meal; to cooking a food because people needed a meal!!
My outlook on food production took on a role of its own, especially as I wanted to learn all I could about aged care cooking.
Different diets needed to be catered for. Whether they be; low fat; diabetic; texture modified; or high calorie fortified foods. The list is endless, and I still can't get enough!
My passion for creating food for people to enjoy can be somewhat intense, but I firmly believe that you CAN have your cake and eat it!!!
My Journey with this type of cooking has led me to try and encourage others to put the love back into their cooking and give people joy at each meal!










{kind=link}