










Warning signs of cognitive declines, like forgetting conversations or missing appointments, might be early signs of Alzheimer’s disease or another type of dementia. they might also represent a treatable condition, like a drug side effect or depression. Either way, it’s important to work out what’s wrong, why it’s happening, and what to try and do. this text provides helpful information on the range of health care providers, including specialists, who may get involved in Alzheimer’s care.
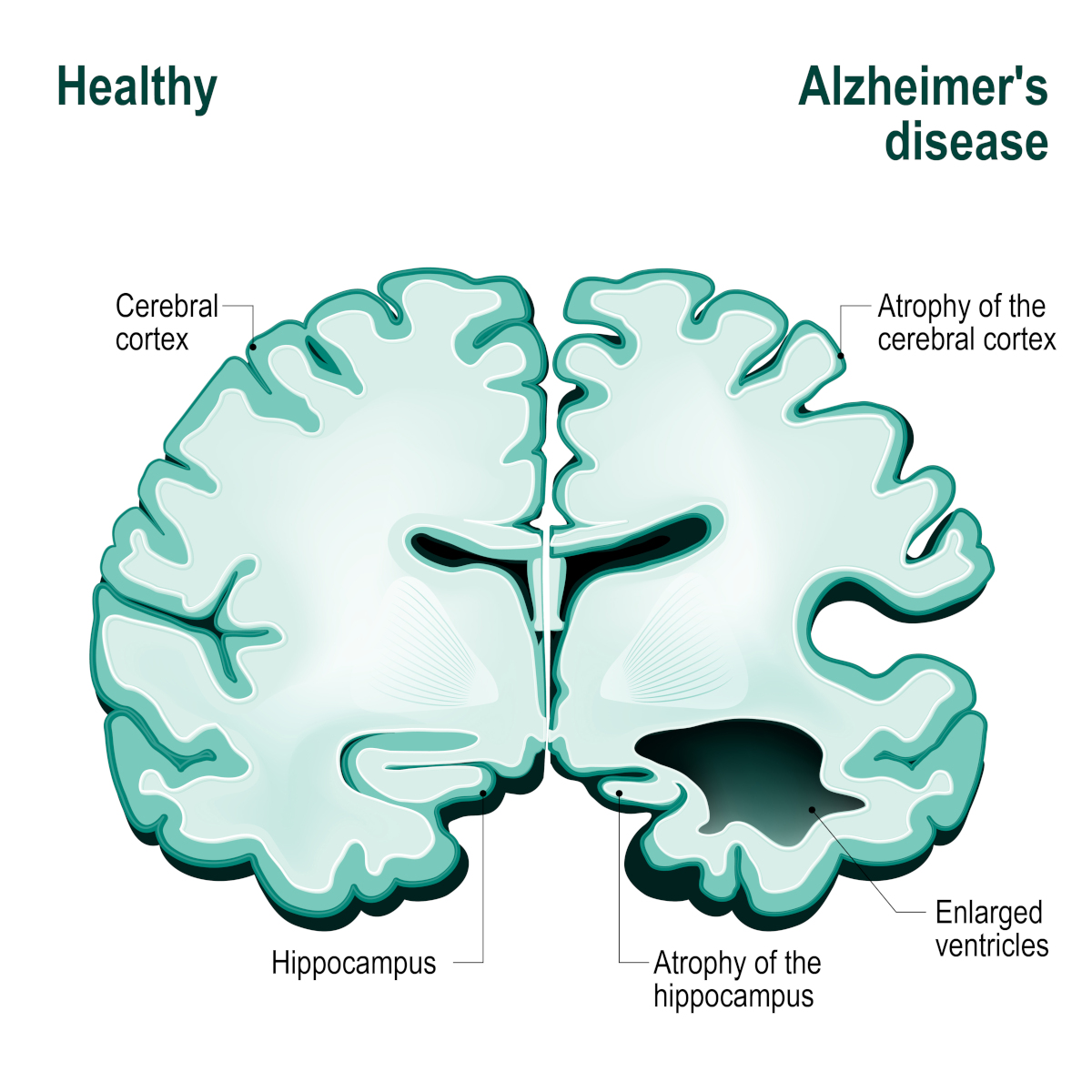 Mr. Thorne’s concerns, unfortunately, are common ones among aging adults—although he’s experiencing his symptoms at an oddly young age. Alzheimer’s disease (AD) and other dementias affect only an occasional percentage of adults in their early 60s, but by age 85 as many as 50% of individuals are affected. Warning signs of cognitive decline, which include symptoms like Mr. Thorne’s, should be taken seriously and not ignored. they will represent treatable conditions like adverse medication effects, substance use, sleep problems, metabolic disorders, or depression. they will even be the first signs of AD or another progressive cognitive disorder. Either way, it’s important to work out what’s wrong, why it’s happening, and what to try doing.
Mr. Thorne’s concerns, unfortunately, are common ones among aging adults—although he’s experiencing his symptoms at an oddly young age. Alzheimer’s disease (AD) and other dementias affect only an occasional percentage of adults in their early 60s, but by age 85 as many as 50% of individuals are affected. Warning signs of cognitive decline, which include symptoms like Mr. Thorne’s, should be taken seriously and not ignored. they will represent treatable conditions like adverse medication effects, substance use, sleep problems, metabolic disorders, or depression. they will even be the first signs of AD or another progressive cognitive disorder. Either way, it’s important to work out what’s wrong, why it’s happening, and what to try doing.
A primary care physician’s (PCP) practice is generally the place to start when questions about cognitive impairment arise, because these symptoms may be connected to other issues in a person’s total health picture. Primary care doctors and nurses are likely to know which initial questions to ask and which screening tests to do.
Depending on the symptoms, they may do a physical examination, draw blood, order imaging studies, and suggest a consultation. Consultation with one of the following specialised professionals, often at the recommendation of a primary care clinician, can be valuable. This is especially true when dealing with a more complicated situation such as a person whose age is young, whose cognitive symptoms are unusual or confusing, whose medical or psychiatric histories are complex, or whose behavioral problems are making it difficult to care for them.
The most common specialists consulted for someone with memory or other cognitive symptoms include the following:
1. Geriatrician
Geriatricians are physicians skilled in assessing and managing the medical problems that affect older adults. they will work as medical aid clinicians or as specialists. Their knowledge of the “geriatric syndromes” like cognitive changes, poly-pharmacy (unraveling the advantages and risks of the multiple medications an older adult can be taking), depression, fatigue, or frailty makes them valuable consultants after you must consider the contributions of medicines and medical illnesses to an older person’s ambiguous symptoms. They take the “broad view” and should put together the massive medical picture especially well.
2. Neurologist
Neurologists are specialists within the diseases of the system. There are many sub-specialty areas in neurology, so make sure to seek out a “cognitive neurologist,” “behavioral neurologist,” or a general neurologist who has experience and expertise in assessing cognitive symptoms. Neurosurgeons aren’t identical as neurologists. they’re experts in operating on the system and are generally consulted after a possible surgical need has been identified. Clinical trials, which can involve testing new medications or diagnostic tools for dementia, often go past a neurologist or a psychiatrist.
3. Psychiatrist
Psychiatrists specialise in the assessment and treatment of mental disorders. Cognitive symptoms board the “gray area” between neurology and psychiatry because they often occur together with behavioral and emotional changes that a psychiatrist is skilled in recognizing and evaluating. Not all psychiatrists are expert evaluators of cognitive disorders, but geriatric psychiatrists specialise in the emotional and behavioral conditions of older adults. Some geriatric psychiatrists and nurse clinical specialists specialise in dementia care, especially within the evaluation and management of behavioral symptoms of dementia-like mood changes, emotional outbursts, agitation, hallucinations or delusions, impulsivity, aggression, and inappropriate behavior.
4. Psychologist
Psychologists are trained to supply various varieties of assessment and psychosocial treatments. Referral to a psychologist could also be made for psychotherapy, including caregiver support. Talk therapy can help an individual and a caregiving system fits the diagnosis of dementia and to deal with sensible concerns, relationship stresses, and emotional reactions that will occur.
5. Neuropsychologist
Many psychologists perform comprehensive evaluations using reliable and standardized tests, and neuropsychologists are the psychologists who are specially trained to judge cognitive disorders. they’re particularly valuable in assessing the severity of blackout or other symptoms, helping to work out the reason behind the symptoms, measuring progress or decline over time, identifying areas of strength which will be reinforced, and designing a non-medication treatment approach.
6. Geriatric Care Manager
Geriatric Care Managers, often trained initially in nursing or welfare work, specialise as “contractors” of geriatric services. they’ll be valuable members of a caregiving team because they’ll assess what social supports are needed so as to cope effectively with present stresses and plans for the long run.
Mr. Thorne’s case illustrates how various health care providers can be involved in his care. He was evaluated by his medical care physician (PCP), who did a cognitive screening examination and identified Mr. Thorne’s cognitive symptoms as significant though mild. After a more thorough assessment, she also worked out that the patient’s fatigue, sleep problems, and forgetfulness had become significant after he was changed to a replacement pressure level medication.
This PCP was very experienced within the care of older adults, so she failed to consider it necessary to urge input from a geriatrician. Blood tests and neuroimaging tests were normal. Mr. Thorne’s symptoms improved only partially after a change in medication, but the PCP asked for neuropsychological testing some months later. The neuropsychologist’s findings, within the context of all the opposite information available, suggested that Mr. Thorne’s difficulties were quite a medicine effect. He was likely experiencing early Alzheimer’s disease.
This was very upsetting news for Mr. Thorne and his wife, and therefore the PCP referred the couple to a geriatric psychiatrist to produce further information about dementia and supportive counseling. A psychiatrist instead of a psychologist was chosen during this case because the PCP suspected Mrs. Thorne might require antidepressant treatment.
The psychiatrist, over several sessions, worked with the couple to facilitate their communication and help them fit this stressful information about Mr. Thorne’s condition. He assessed Mrs. Thorne for depression and a choice was made to defer medication treatment for her symptoms, which appeared to be a brief adjustment. He discussed the pros and cons of currently available AD medications for Mr. Thorne and gave the Thornes information regarding clinical trials that may be appropriate for Mr. Thorne to think about.
The psychiatrist then referred them to a geriatric care manager who assisted them in planning for a future when additional supports might become necessary regarding financial planning, residential considerations, transportation, and advance care planning.
Resources:










{kind=link}